When is the booster administered?
Across the world, including in Sri Lanka, the booster is given three months after the second dose of the original regime.
Who can get a COVID booster in Sri Lanka?
At the time of writing, the Ministry of Health is rolling out the booster program for:
- Healthcare and front line workers
- Over 60 population
- Those who are 20 years and above with comorbidities or are immunocompromised (at least after one month after the second dose)
The booster is currently given to those above 60 in the Southern & Western provinces, Anuradhapura and Ampara. They will receive an SMS with the date, time and location of the booster.
Which vaccine is used as a booster in Sri Lanka?
Pfizer/BioNTech mRNA vaccine (30mg dosage) is used as a booster in Sri Lanka. This method of mixing different vaccines (heterologous booster) has been previously used for other vaccines such as Ebola.
Wait, but I got AstraZeneca as my first two doses. Is it safe to mix & match?
Short answer: Yes.
Long answer: In May 2021, a UK trial(3) of 830 participants reported safety data for mix & match vaccines when compared to same type (homologous) vaccines. Though those that received Pfizer after AstraZeneca reported greater intensity of fatigue, headaches and muscle aches – these side effects only lasted 48 hours. There were no hospitalisations or any severe adverse events reported.
What about Sinopharm?
There have been no published studies on mixing mRNA vaccines with Sinopharm. However, Bahrain started boosting those that received two doses of Sinopharm with Pfizer in June.
Are we the only country mixing and matching vaccines?
Nope! Pfizer and Moderna have been approved as booster doses for those that have taken other vaccines in major countries such as the U.K, U.S, Canada and Israel.
Okay, say I get this booster. What does it mean for my immunity against COVID-19?
The Spanish CombiVac trial(2) with 663 people reported in May 2021 that the participants who received a Pfizer booster eight weeks after receiving their first AstraZeneca dose showed a markedly higher level of antibodies than the response generated after two doses of AstraZeneca.
This is expected. When additional doses of a viral vaccine like AZ is administered, the body generates an immune response quickly to destroy the foreign particles. Basically, it becomes good at recognising the virus that it doesn’t allow the vaccine to do its thing – last long enough in the body to actually boost the immune response.
However, by introducing an mRNA vaccine after a viral vaccine, the body is made to work a little harder and longer to recognise the virus. This results in a boosted immune response.
Okay but how many boosters will we need? Will this pandemic ever end?
This too shall pass so the pandemic will end. However, we have a large role to play in this. Our behaviour will dictate whether the pandemic rages on with newer and more potent variants or it gets squashed sooner than later. Variants occur when the virus is allowed to spread so stopping the spread by sticking to COVID19 guidelines is of paramount importance. The less variants, the less need for boosters.
Vaccines save lives and vaccinated people don’t spread the virus as easily as unvaccinated people. So the more people that get vaccinated, the less spread and the sooner we can end this merry go round.
Got more questions? Want to understand whether you should sign yourself or your loved one up for a booster dose? Speak to one of our doctors on oDoc! Download the app today!
Sources
- Booster Shots and Third Doses for COVID19 Vaccines: Everything You Need to Know. (2021)., Johns Hopkins Medicine
- Callaway, E (2021), Mix-and-match COVID vaccines trigger potent immune response., Nature.
- Shaw, R et al (2021)., Heterologous prime-boost COVID19 vaccination: initial reactogenicity data., The Lancet., 397:2043-2046
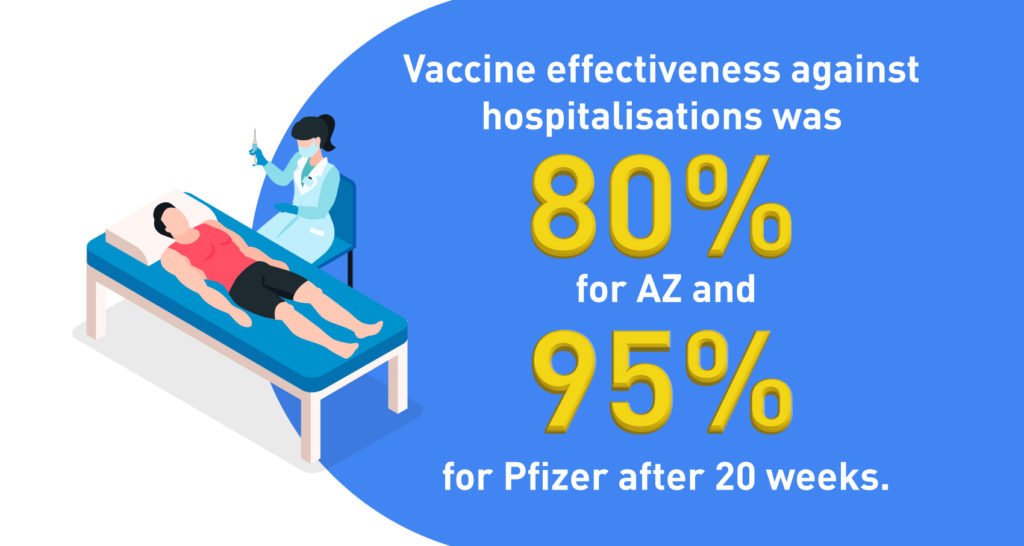
- Duration of protection of COVID-19 vaccines against clinical disease. (2021) Public Health England
- Bernal et al (2021)., Effectiveness of COVID-19 vaccines against the Delta variant., NEJM., 385:585-594